Congenital cysts can develop in the lungs of infants. In this article, you will find information about the different types of these cysts, how they are diagnosed, monitored, and treated. There are three main types of congenital lung cysts: Congenital Cystic Adenomatoid Malformations (CCAM), Pulmonary Sequestration, and Congenital Lobar Emphysema.
Congenital Cystic Adenomatoid Malformation (CCAM)
The most common congenital cystic lung disease is known as Congenital Cystic Adenomatoid Malformation (CCAM). Each year, approximately 50 babies are born with this condition in our country.
During fetal development, abnormal branching of the bronchial airways can result in cysts of various sizes.
The cause of CCAM formation is unknown.
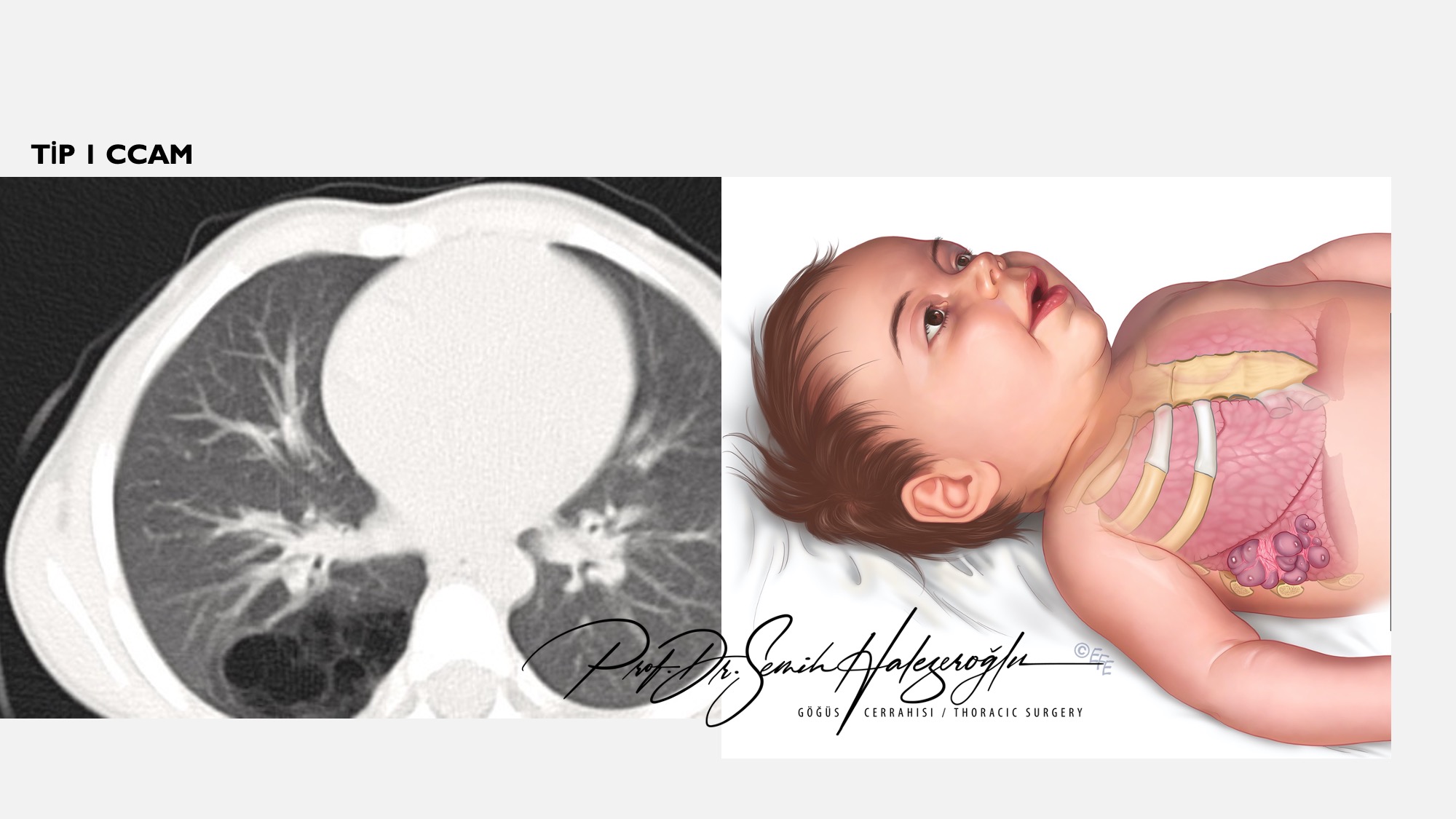
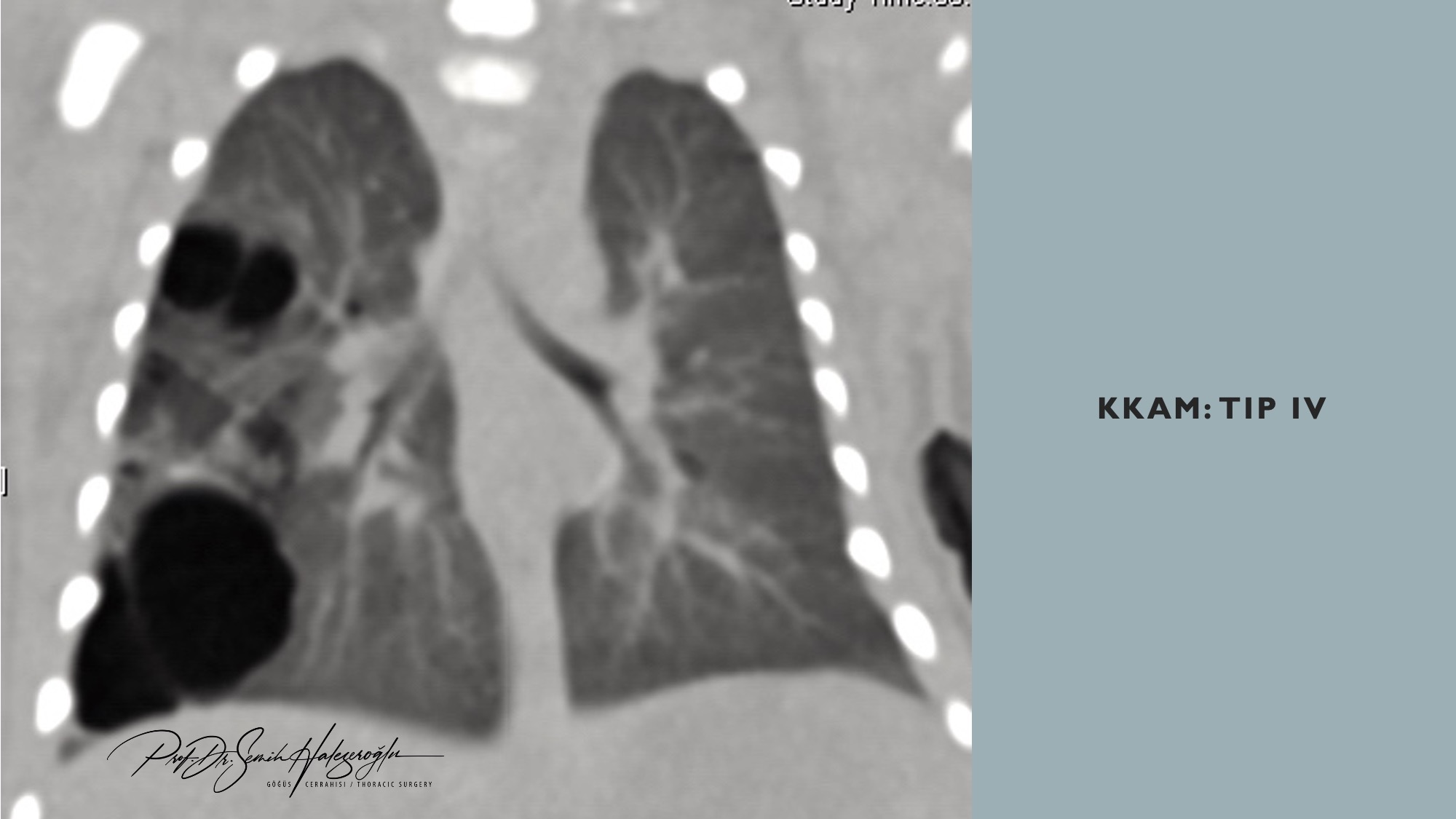
Depending on the number and size of the cysts, they are classified into five types: Type 0, 1, 2, 3, and 4.
How Is CCAM Diagnosed?
It is typically detected during ultrasounds performed after the 24th week of pregnancy. Depending on the size of the cysts, displacement of the baby’s heart may be observed. However, this condition usually does not pose any significant problems for the baby’s development in the womb. Subsequent ultrasounds may show that the cysts shrink, remain the same, or grow.
When CCAM Is Detected in the Womb
Families should not be overly concerned about CCAM. Termination of pregnancy due to CCAM is very rare and only considered necessary in cases where a condition known as hydrops develops. This is determined by the specialist doctors monitoring the mother. However, most babies with CCAM are expected to be born healthy. It is still advisable for the birth to take place in a well-equipped hospital due to the potential for respiratory issues at birth.
Postnatal Procedures
Following birth, the baby is kept under observation by pediatric specialists at the hospital. As previously mentioned, significant respiratory issues are generally not observed in such cases. During this period, a CT scan of the lungs is performed to obtain a more detailed view of the cysts previously detected during ultrasound.
Below are CT images from some of our patients with CCAM.

The first postnatal CT scan is crucial for monitoring the baby’s condition. If any symptoms such as difficulty feeding, unusual crying, discoloration, or other issues arise in the following months, or if pediatric evaluations raise concerns, a new CT scan is conducted for comparison, and a treatment decision is made.
However, in the majority of cases, no significant symptoms appear. In such instances, a new CT scan is performed when the baby is 11 months old to assess the status of the cysts based on the initial scan.
CCAM Treatment
Cysts resulting from Congenital Cystic Adenomatoid Malformation can lead to frequent respiratory infections once the baby starts moving around after the age of one. These infections tend to become more frequent as the child grows, negatively impacting their development. Additionally, medical literature indicates that these cysts have the potential to develop into malignancies called blastomas. Therefore, CCAM is a condition that requires treatment and should not be merely monitored. There are no drug treatments available for CCAM.
CCAM Surgery
Not all CCAM cases identified before or shortly after birth require surgery. Based on our experience, about 20% of babies with CCAM visible in postnatal CT scans show regression in follow-up scans at 11 months. These cases can be managed with monitoring by a pediatric specialist. However, surgery is necessary in 80% of cases.
Open CCAM Surgery

In open surgeries, a long incision is made on the side of the chest, the ribs are separated, and the affected lung lobe containing the cysts is removed. After surgery, babies are monitored in intensive care before being transferred to regular care.
As seen in the image, open surgeries are now only performed when absolutely necessary.
Minimally Invasive CCAM Surgery
Over the years, as surgeons have gained more experience and medical technology has advanced, these surgeries have transitioned to minimally invasive methods. These procedures, also known as minimally invasive surgeries, avoid opening the chest cavity and offer numerous advantages: less damage to the patient, reduced postoperative pain, minimal need for intensive care, shorter hospital stays (average 3 days), and small incisions.
These surgeries can be performed in infants as early as six months of age when necessary.

Minimally invasive lung surgeries in infants are performed only in advanced centers by experienced pediatric or thoracic surgeons.
Pulmonary Sequestration
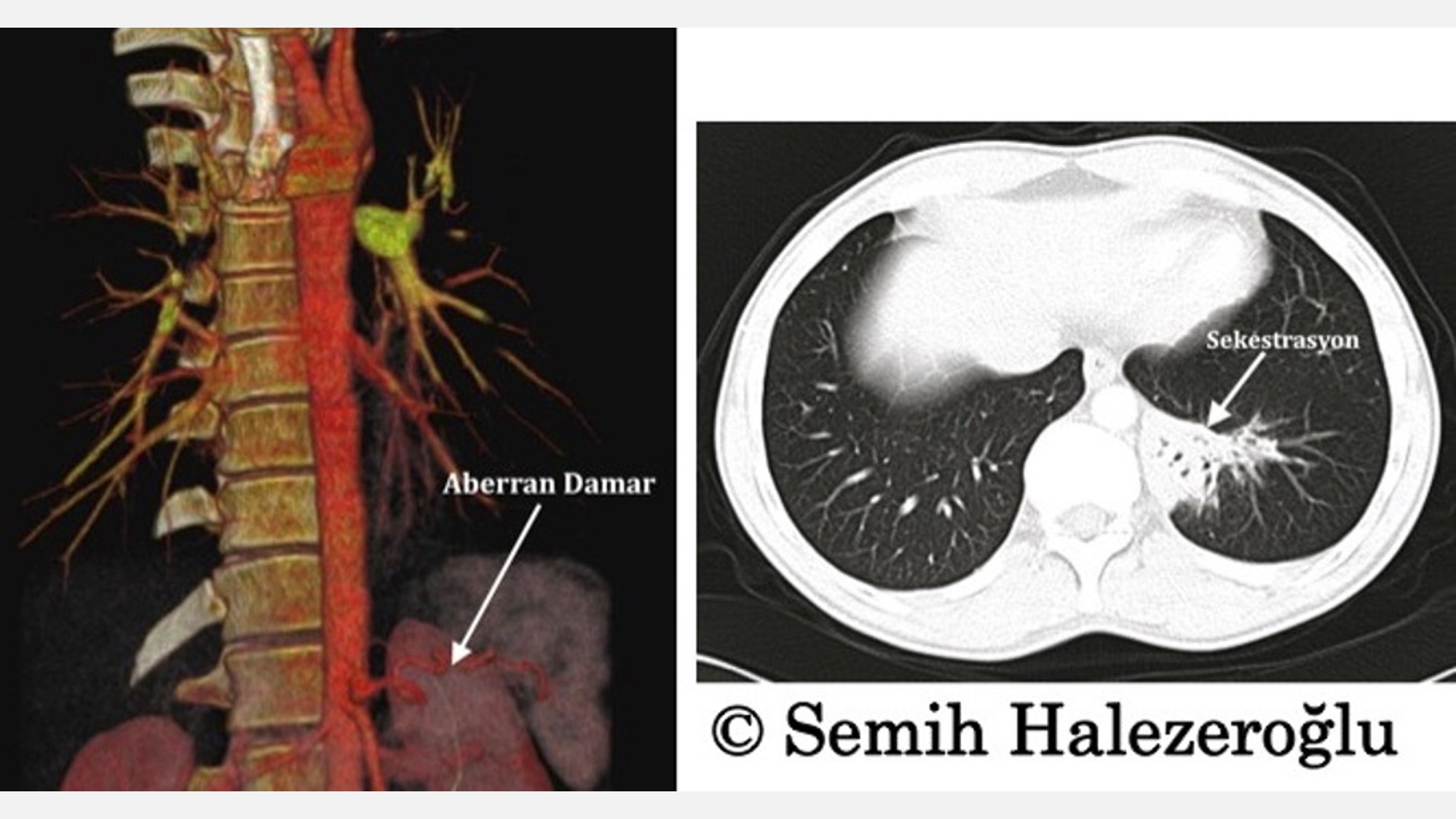
Pulmonary sequestration is a less common type of congenital lung cyst compared to CCAM. This condition is caused by an aberrant artery from the aorta, the body’s largest artery, supplying a portion of the lung. Due to the lung’s structure not being suited for such an artery, excessive blood flow leads to damage and cyst formation. Infections and bleeding within these cysts can compromise the patient’s health.
Contrast-enhanced CT scans that reveal this aberrant artery indicate the need for surgery, which can be performed using minimally invasive methods after six months of age.
Pulmonary Sequestration Surgery
Preoperative CT scans identify the aberrant artery supplying the lung. One of the most critical parts of the surgery is safely closing off this artery. Once this is done, the lung lobe containing the cysts is removed using minimally invasive techniques.
Post-surgery, patients typically stay in the hospital for 3 to 4 days.
Minimally invasive surgery for pulmonary sequestration has a high success rate when performed by experienced surgeons in advanced centers.
The video below shows the procedure in action.
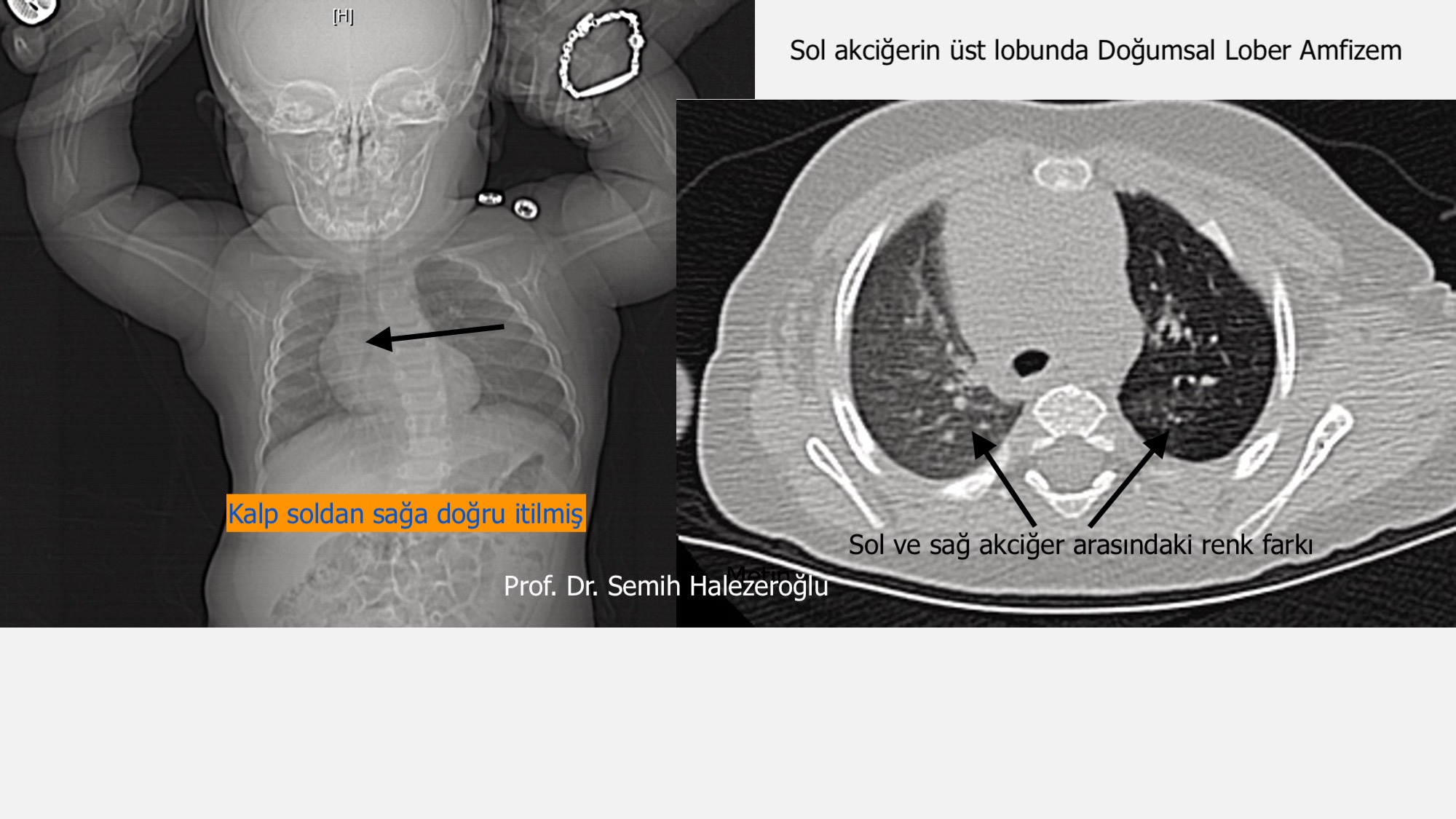
Congenital Lobar Emphysema
Although classified among congenital cystic lung diseases, cysts are rarely observed in Congenital Lobar Emphysema. This condition occurs due to abnormalities in the cartilage of the bronchi. During inhalation, air enters the lungs, but during exhalation, the bronchi collapse, trapping air. This trapped air causes the affected lung to overinflate, pressing against the heart and major blood vessels, leading to shortness of breath during exertion and increased heart rate.
Different severity levels of congenital lobar emphysema determine whether treatment or monitoring is necessary. Surgery is performed only in infants with significant symptoms.